
When a thermographer has an inquiry from someone who is pregnant or actively breastfeeding the thermographer is sometimes not sure what to say.
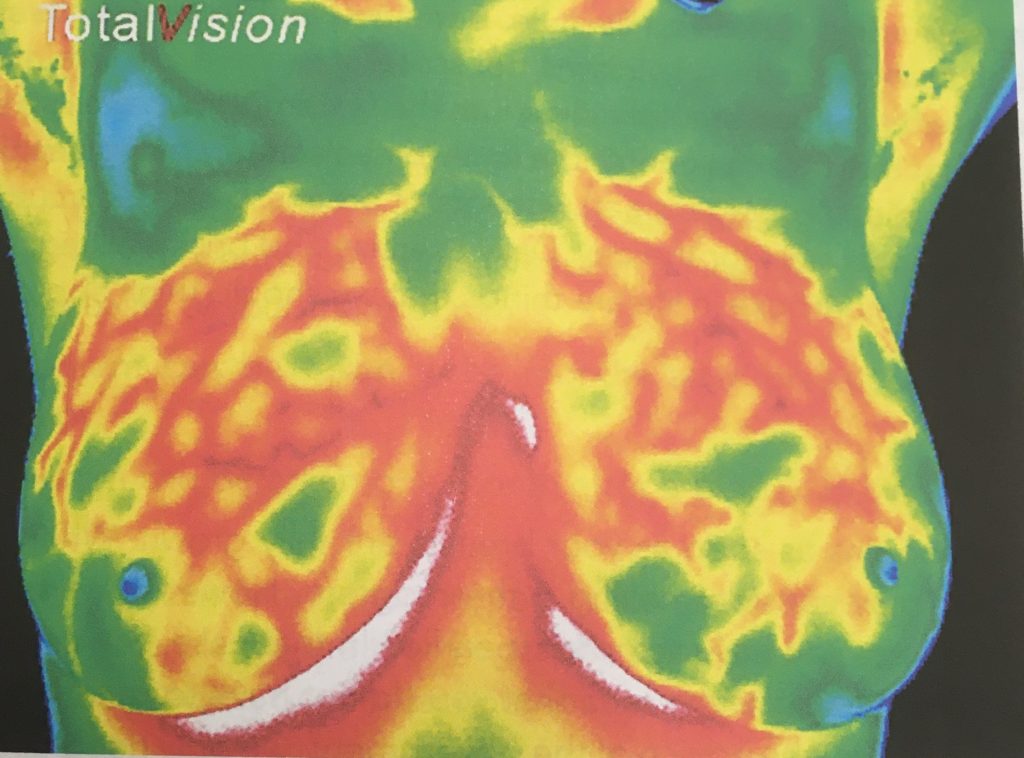
Because the breast becomes naturally hyper-vascular, preparing for childbirth, the evaluation becomes complicated or challenging for the interpreter. This process in the breast begins almost immediately after conception, possibly within weeks and continues until the mother ceases to breast feed. Even then the breasts do not usually return to a “normal” state for a few months after that.
My recommendation is that of course, this is not a good time to create a baseline, but if the woman is having a worrying pain, a lump or something unusual, on one side only, then a thermogram MAY offer some beneficial information.
My experience is that she will seek a thermogram to alleviate fears and may be reluctant to see her doctor, especially if she wants to continue breastfeeding. However, the best advice is an examination with her doctor even before the imaging.
What would the interpreter be looking for? If there is a lump, the interpreter would need to know the exact location of the lump or region of concern with a clear description as to approximate size and movability, etc., so there could be a thermal evaluation at that exact location. Still, it is not uncommon that it could possibly be a clogged milk duct.
Typically, both breasts will be hyper-vascular but if lactating, the baby, or mother will prefer one breast over the other, creating more activity on that breast, which is something the interpreter needs to know as well. For this reason, assessing asymmetry is not the best indication of a thermal abnormality.
Bottom line, I would only accept an appointment if there was a significant concern in one breast. I would also advise the client that is it’s a challenging evaluation, but the interpreter will do their best with an abundance of information regarding the concern and will likely recommend a visit with her doctor.
It would be best if we had a previous breast evaluation before pregnancy (maybe a good reason for younger women to have a baseline) and it would also be best to schedule a non-lactating follow-up three months after weaning.
Carol Chandler D.O.M.

{kind=link}
{kind=link}